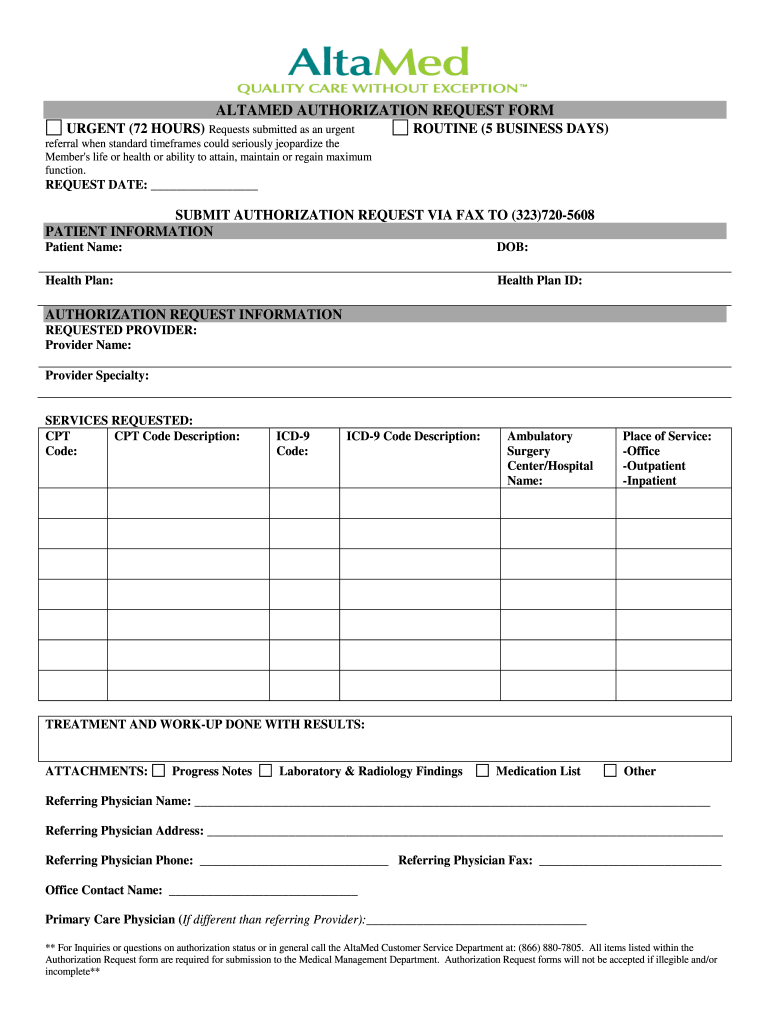
Altamed Authorization Form - Fill out the patient and request information, attach. I hereby authorize altamed health services corporation to disclose confidential sensitive health information to the person/organization. If you choose to do so, it must be done in writing and signed by you or your legal representative and sent to the following address: Enhanced care management (ecm) authorization for the use and disclosure of health and social information | english Download a pdf file of the altamed authorization request form for urgent or routine referrals.
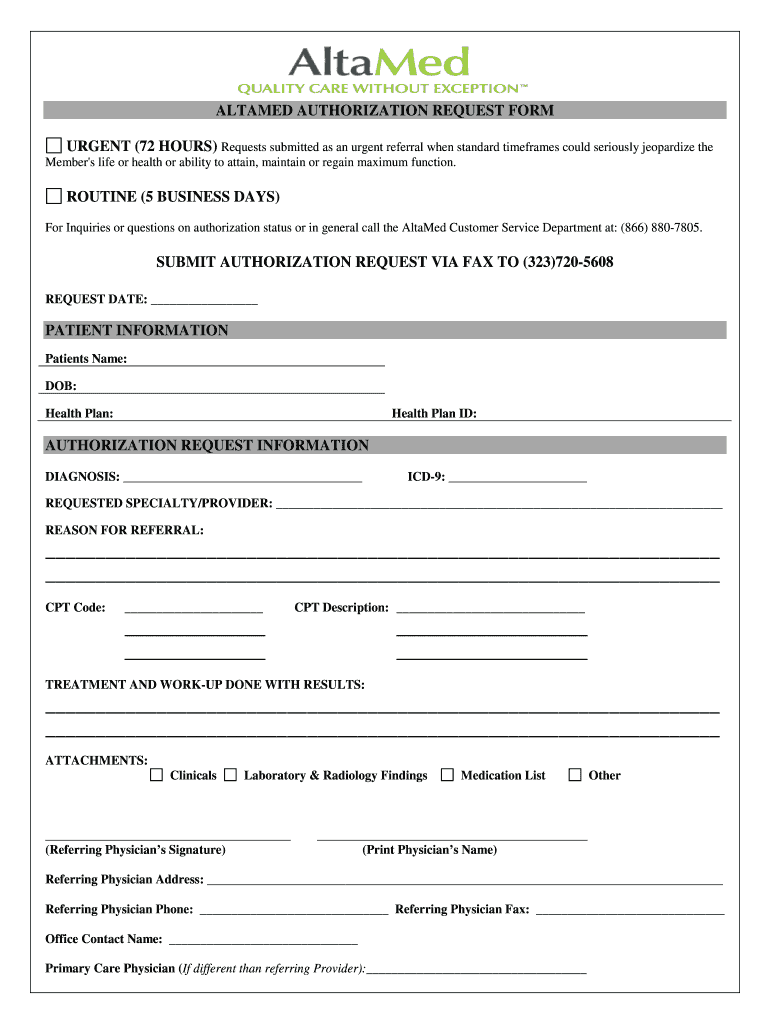
Download a pdf file of the altamed authorization request form for urgent or routine referrals. Fill out the patient and request information, attach. Enhanced care management (ecm) authorization for the use and disclosure of health and social information | english If you choose to do so, it must be done in writing and signed by you or your legal representative and sent to the following address: I hereby authorize altamed health services corporation to disclose confidential sensitive health information to the person/organization.
Fill out the patient and request information, attach. I hereby authorize altamed health services corporation to disclose confidential sensitive health information to the person/organization. Download a pdf file of the altamed authorization request form for urgent or routine referrals. If you choose to do so, it must be done in writing and signed by you or your legal representative and sent to the following address: Enhanced care management (ecm) authorization for the use and disclosure of health and social information | english
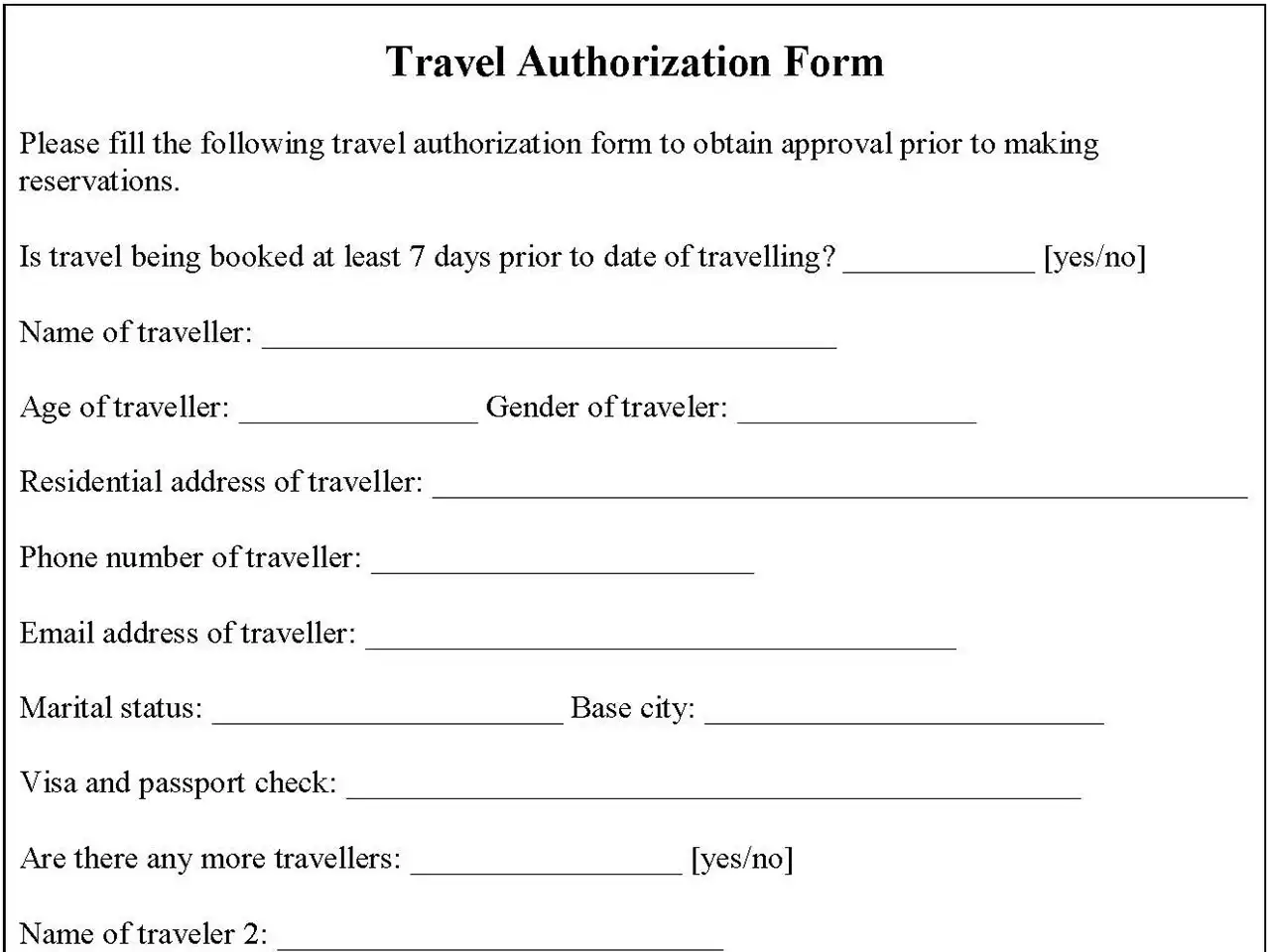
Travel Authorization Form Editable PDF Forms
Download a pdf file of the altamed authorization request form for urgent or routine referrals. Fill out the patient and request information, attach. I hereby authorize altamed health services corporation to disclose confidential sensitive health information to the person/organization. Enhanced care management (ecm) authorization for the use and disclosure of health and social information | english If you choose to.
Form Altamed ≡ Fill Out Printable PDF Forms Online
If you choose to do so, it must be done in writing and signed by you or your legal representative and sent to the following address: Enhanced care management (ecm) authorization for the use and disclosure of health and social information | english I hereby authorize altamed health services corporation to disclose confidential sensitive health information to the person/organization. Download.
Altamed Authorization Form Fill Online, Printable, Fillable, Blank
Download a pdf file of the altamed authorization request form for urgent or routine referrals. Fill out the patient and request information, attach. Enhanced care management (ecm) authorization for the use and disclosure of health and social information | english If you choose to do so, it must be done in writing and signed by you or your legal representative.
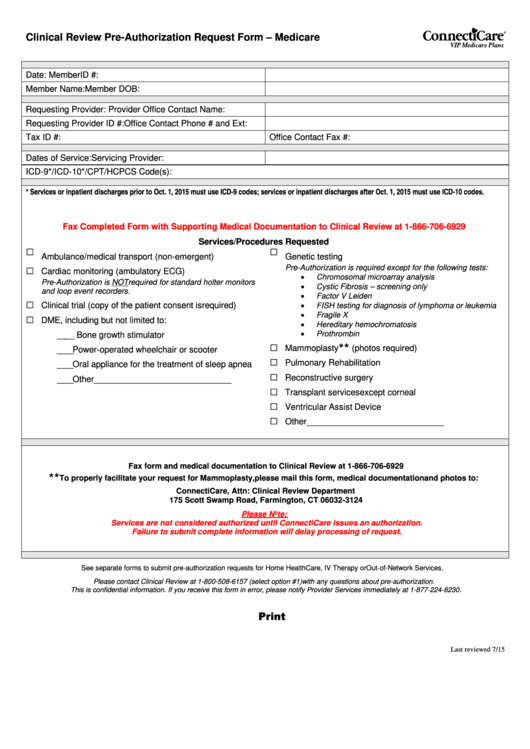
Clinical Review PreAuthorization Request Form Medicare printable pdf
Fill out the patient and request information, attach. Download a pdf file of the altamed authorization request form for urgent or routine referrals. I hereby authorize altamed health services corporation to disclose confidential sensitive health information to the person/organization. Enhanced care management (ecm) authorization for the use and disclosure of health and social information | english If you choose to.
Fillable Online Altamed Prior Authorization Form tabu.renove.it Fax
I hereby authorize altamed health services corporation to disclose confidential sensitive health information to the person/organization. Fill out the patient and request information, attach. Enhanced care management (ecm) authorization for the use and disclosure of health and social information | english If you choose to do so, it must be done in writing and signed by you or your legal.
Fillable Online Altamed Authorization Form Fill Online, Printable
Enhanced care management (ecm) authorization for the use and disclosure of health and social information | english If you choose to do so, it must be done in writing and signed by you or your legal representative and sent to the following address: Fill out the patient and request information, attach. I hereby authorize altamed health services corporation to disclose.

Authorization Form Stock Illustration Download Image Now Abstract
Download a pdf file of the altamed authorization request form for urgent or routine referrals. I hereby authorize altamed health services corporation to disclose confidential sensitive health information to the person/organization. If you choose to do so, it must be done in writing and signed by you or your legal representative and sent to the following address: Enhanced care management.
Altura authorization request form Fill out & sign online DocHub
If you choose to do so, it must be done in writing and signed by you or your legal representative and sent to the following address: Fill out the patient and request information, attach. I hereby authorize altamed health services corporation to disclose confidential sensitive health information to the person/organization. Download a pdf file of the altamed authorization request form.
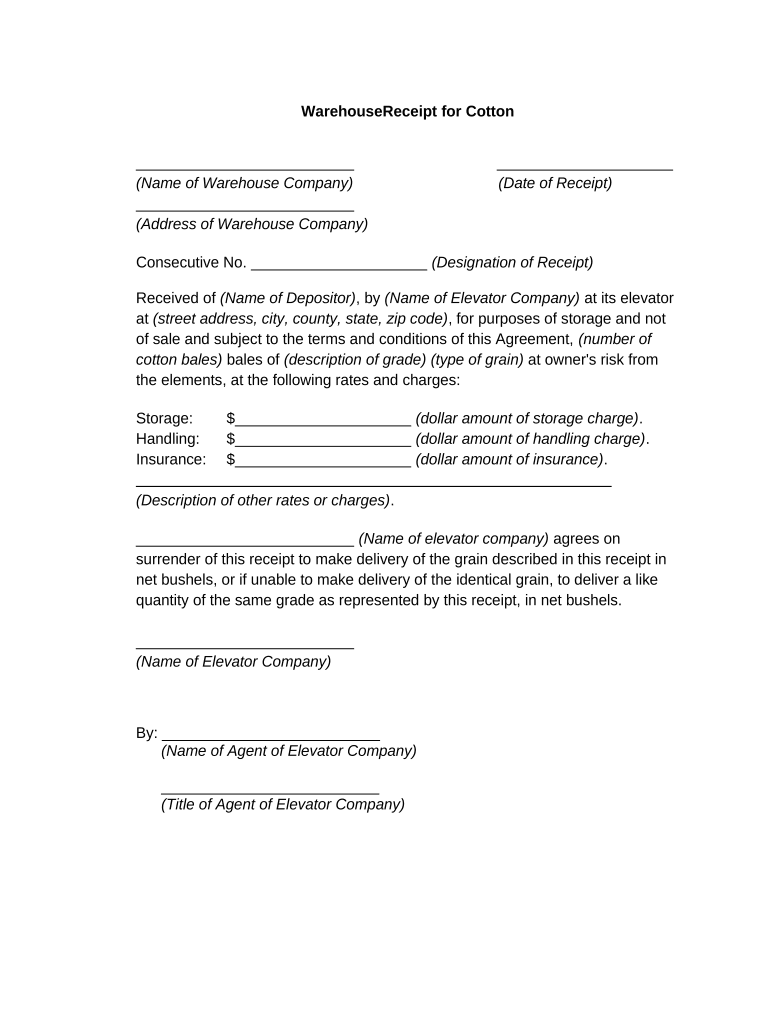
Warehouse Receipt for Cotton Form Fill Out and Sign Printable PDF
I hereby authorize altamed health services corporation to disclose confidential sensitive health information to the person/organization. If you choose to do so, it must be done in writing and signed by you or your legal representative and sent to the following address: Enhanced care management (ecm) authorization for the use and disclosure of health and social information | english Download.
Direct deposit authorization form in Word and Pdf formats
Download a pdf file of the altamed authorization request form for urgent or routine referrals. If you choose to do so, it must be done in writing and signed by you or your legal representative and sent to the following address: Fill out the patient and request information, attach. I hereby authorize altamed health services corporation to disclose confidential sensitive.
If You Choose To Do So, It Must Be Done In Writing And Signed By You Or Your Legal Representative And Sent To The Following Address:
Enhanced care management (ecm) authorization for the use and disclosure of health and social information | english I hereby authorize altamed health services corporation to disclose confidential sensitive health information to the person/organization. Download a pdf file of the altamed authorization request form for urgent or routine referrals. Fill out the patient and request information, attach.