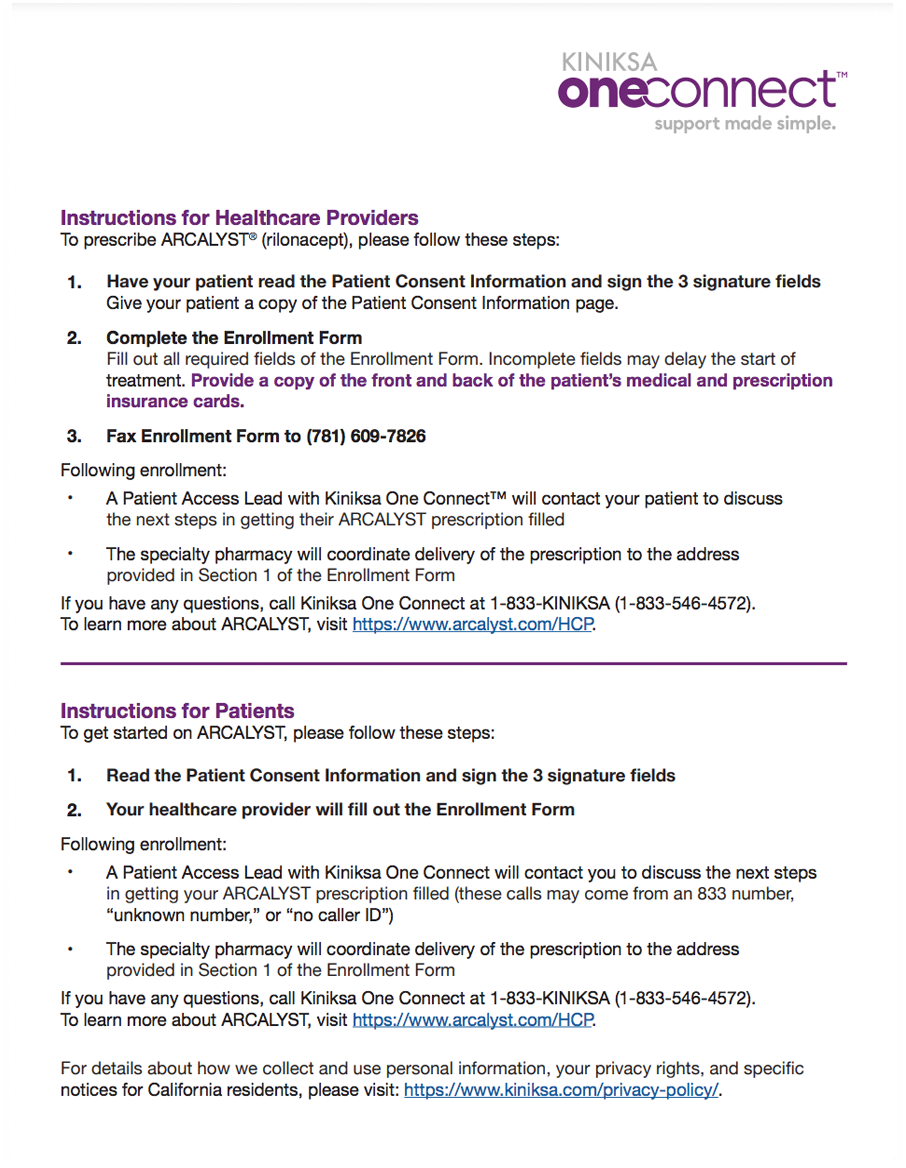
Arcalyst Enrollment Form - By completing an enrollment form, your patient may be eligible to receive kiniksa oneconnect™ program benefits, such as financial assistance. After your healthcare provider submits a kiniksa oneconnect ™ enrollment form with your signature as consent, our work begins. Arcalyst na please complete an arcalyst patient enrollment and consent form and indicate cvs specialty as your preferred pharmacy provider. Your healthcare provider will fill out the enrollment form following enrollment: • a patient access lead with kiniksa one connect will contact you. The primary purpose of this form is to streamline the enrollment process for patients seeking arcalyst therapy. • a patient access lead with the kiniksa oneconnect™ program will contact. Treatment of recurrent pericarditis (rp) and reduction in risk of.
Treatment of recurrent pericarditis (rp) and reduction in risk of. The primary purpose of this form is to streamline the enrollment process for patients seeking arcalyst therapy. By completing an enrollment form, your patient may be eligible to receive kiniksa oneconnect™ program benefits, such as financial assistance. • a patient access lead with the kiniksa oneconnect™ program will contact. Arcalyst na please complete an arcalyst patient enrollment and consent form and indicate cvs specialty as your preferred pharmacy provider. Your healthcare provider will fill out the enrollment form following enrollment: After your healthcare provider submits a kiniksa oneconnect ™ enrollment form with your signature as consent, our work begins. • a patient access lead with kiniksa one connect will contact you.
• a patient access lead with kiniksa one connect will contact you. After your healthcare provider submits a kiniksa oneconnect ™ enrollment form with your signature as consent, our work begins. By completing an enrollment form, your patient may be eligible to receive kiniksa oneconnect™ program benefits, such as financial assistance. Treatment of recurrent pericarditis (rp) and reduction in risk of. The primary purpose of this form is to streamline the enrollment process for patients seeking arcalyst therapy. Your healthcare provider will fill out the enrollment form following enrollment: • a patient access lead with the kiniksa oneconnect™ program will contact. Arcalyst na please complete an arcalyst patient enrollment and consent form and indicate cvs specialty as your preferred pharmacy provider.

Junior High School Enrollment Form Excel Template And Google Sheets
Your healthcare provider will fill out the enrollment form following enrollment: After your healthcare provider submits a kiniksa oneconnect ™ enrollment form with your signature as consent, our work begins. • a patient access lead with kiniksa one connect will contact you. • a patient access lead with the kiniksa oneconnect™ program will contact. Arcalyst na please complete an arcalyst.

Resources/FAQ
By completing an enrollment form, your patient may be eligible to receive kiniksa oneconnect™ program benefits, such as financial assistance. Your healthcare provider will fill out the enrollment form following enrollment: After your healthcare provider submits a kiniksa oneconnect ™ enrollment form with your signature as consent, our work begins. The primary purpose of this form is to streamline the.
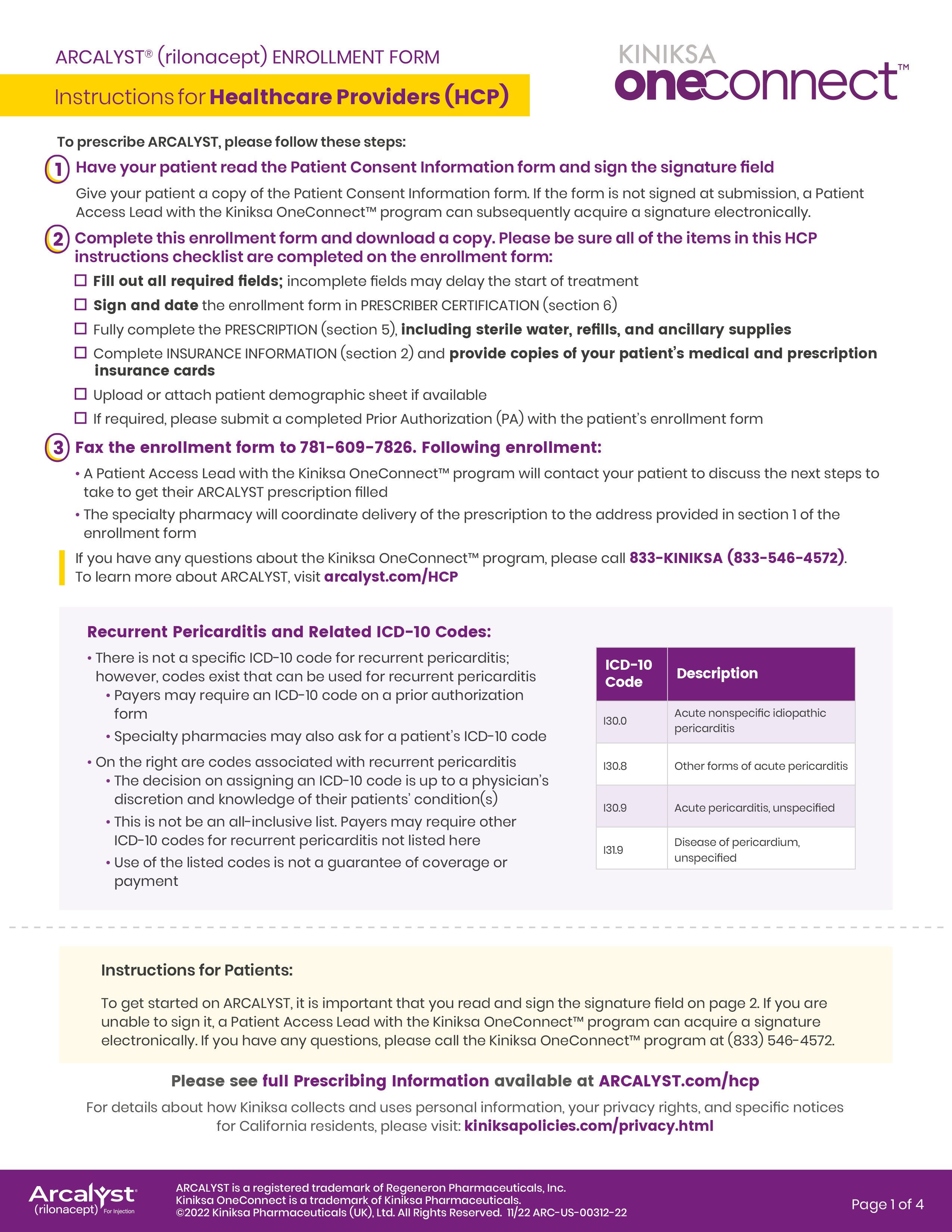
Access and Support ARCALYST (rilonacept)
Your healthcare provider will fill out the enrollment form following enrollment: By completing an enrollment form, your patient may be eligible to receive kiniksa oneconnect™ program benefits, such as financial assistance. After your healthcare provider submits a kiniksa oneconnect ™ enrollment form with your signature as consent, our work begins. Arcalyst na please complete an arcalyst patient enrollment and consent.
Access and Support ARCALYST (rilonacept)
Your healthcare provider will fill out the enrollment form following enrollment: Treatment of recurrent pericarditis (rp) and reduction in risk of. After your healthcare provider submits a kiniksa oneconnect ™ enrollment form with your signature as consent, our work begins. Arcalyst na please complete an arcalyst patient enrollment and consent form and indicate cvs specialty as your preferred pharmacy provider..
Enroll, 3d rendering, rough street sign collection. , 3d rendering
By completing an enrollment form, your patient may be eligible to receive kiniksa oneconnect™ program benefits, such as financial assistance. Your healthcare provider will fill out the enrollment form following enrollment: Arcalyst na please complete an arcalyst patient enrollment and consent form and indicate cvs specialty as your preferred pharmacy provider. • a patient access lead with kiniksa one connect.
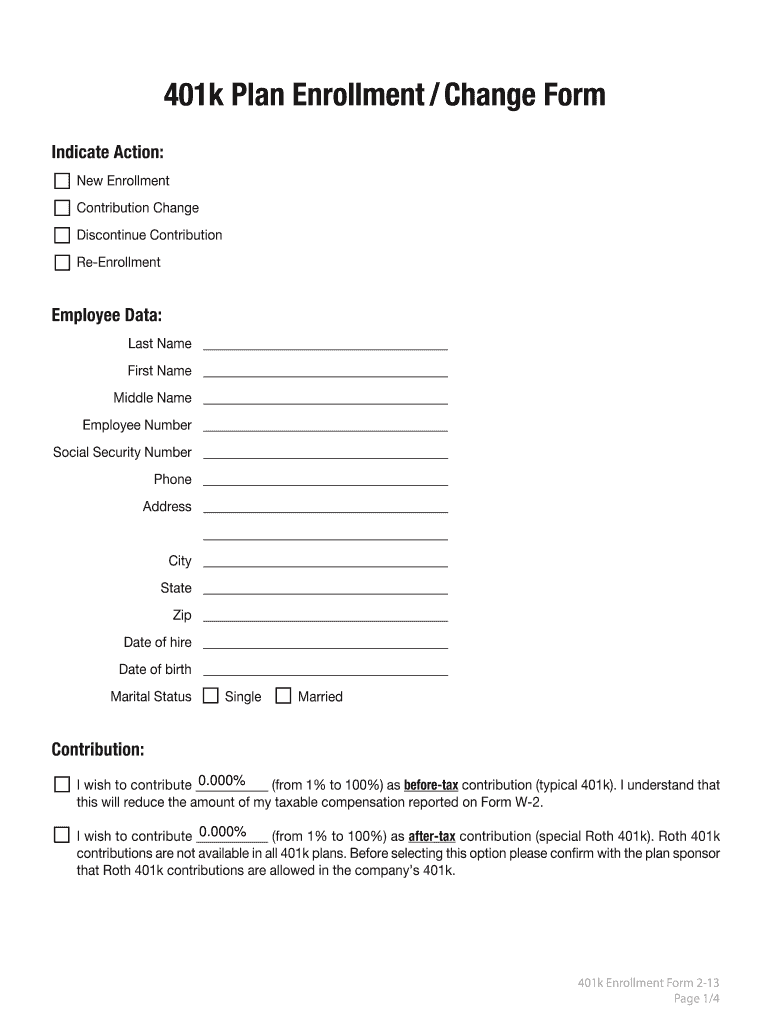
401k Enrollment Form 2 13 AI 401k Network Fill Out and Sign Printable
By completing an enrollment form, your patient may be eligible to receive kiniksa oneconnect™ program benefits, such as financial assistance. • a patient access lead with kiniksa one connect will contact you. Your healthcare provider will fill out the enrollment form following enrollment: • a patient access lead with the kiniksa oneconnect™ program will contact. Arcalyst na please complete an.

Enrollment Photos Philippine News Agency
By completing an enrollment form, your patient may be eligible to receive kiniksa oneconnect™ program benefits, such as financial assistance. • a patient access lead with the kiniksa oneconnect™ program will contact. Your healthcare provider will fill out the enrollment form following enrollment: After your healthcare provider submits a kiniksa oneconnect ™ enrollment form with your signature as consent, our.

Pricing Melita Group
The primary purpose of this form is to streamline the enrollment process for patients seeking arcalyst therapy. • a patient access lead with the kiniksa oneconnect™ program will contact. By completing an enrollment form, your patient may be eligible to receive kiniksa oneconnect™ program benefits, such as financial assistance. Treatment of recurrent pericarditis (rp) and reduction in risk of. After.
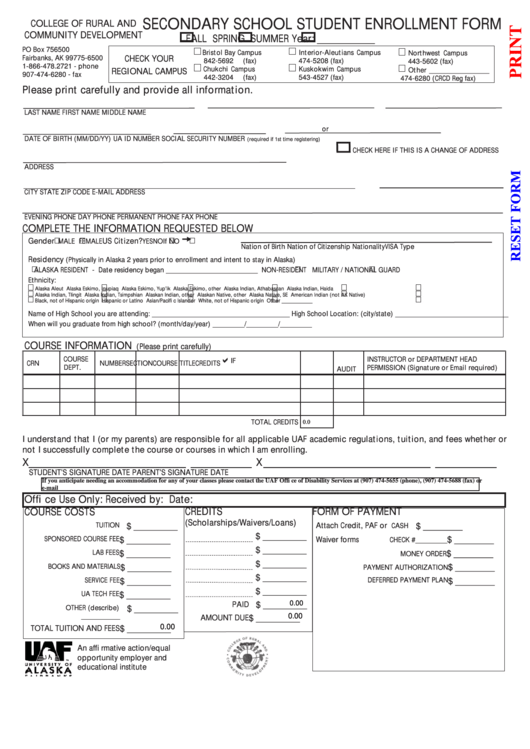
9th Enrollment Form Pdf Enrollment Form
• a patient access lead with kiniksa one connect will contact you. Arcalyst na please complete an arcalyst patient enrollment and consent form and indicate cvs specialty as your preferred pharmacy provider. Your healthcare provider will fill out the enrollment form following enrollment: After your healthcare provider submits a kiniksa oneconnect ™ enrollment form with your signature as consent, our.
Enrollment Fee
Arcalyst na please complete an arcalyst patient enrollment and consent form and indicate cvs specialty as your preferred pharmacy provider. Treatment of recurrent pericarditis (rp) and reduction in risk of. By completing an enrollment form, your patient may be eligible to receive kiniksa oneconnect™ program benefits, such as financial assistance. Your healthcare provider will fill out the enrollment form following.
Treatment Of Recurrent Pericarditis (Rp) And Reduction In Risk Of.
Arcalyst na please complete an arcalyst patient enrollment and consent form and indicate cvs specialty as your preferred pharmacy provider. • a patient access lead with the kiniksa oneconnect™ program will contact. The primary purpose of this form is to streamline the enrollment process for patients seeking arcalyst therapy. By completing an enrollment form, your patient may be eligible to receive kiniksa oneconnect™ program benefits, such as financial assistance.
After Your Healthcare Provider Submits A Kiniksa Oneconnect ™ Enrollment Form With Your Signature As Consent, Our Work Begins.
• a patient access lead with kiniksa one connect will contact you. Your healthcare provider will fill out the enrollment form following enrollment: