Dental Records Request Form - Patient authorization to transfer or forward dental records i, , hereby request and authorize patient or guardian name (please print). The patient’s request must be in writing, signed by the patient, and clearly identify the designated person and where to send the copied records.
Patient authorization to transfer or forward dental records i, , hereby request and authorize patient or guardian name (please print). The patient’s request must be in writing, signed by the patient, and clearly identify the designated person and where to send the copied records.
The patient’s request must be in writing, signed by the patient, and clearly identify the designated person and where to send the copied records. Patient authorization to transfer or forward dental records i, , hereby request and authorize patient or guardian name (please print).

Dental Records Release Form Template Rumina Rahija
Patient authorization to transfer or forward dental records i, , hereby request and authorize patient or guardian name (please print). The patient’s request must be in writing, signed by the patient, and clearly identify the designated person and where to send the copied records.
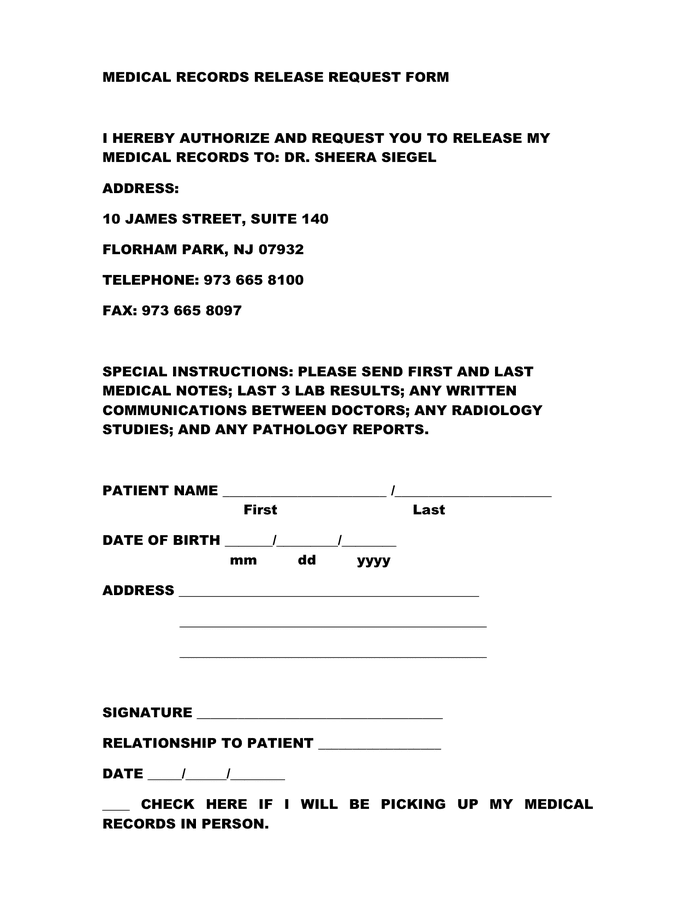
Medical records release request form in Word and Pdf formats
The patient’s request must be in writing, signed by the patient, and clearly identify the designated person and where to send the copied records. Patient authorization to transfer or forward dental records i, , hereby request and authorize patient or guardian name (please print).
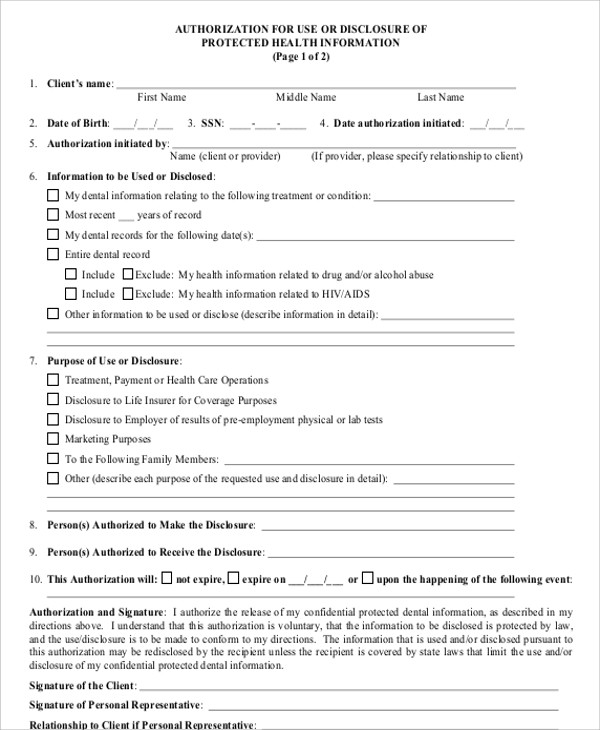
Free Printable Dental Hipaa Forms Printable Word Searches
The patient’s request must be in writing, signed by the patient, and clearly identify the designated person and where to send the copied records. Patient authorization to transfer or forward dental records i, , hereby request and authorize patient or guardian name (please print).
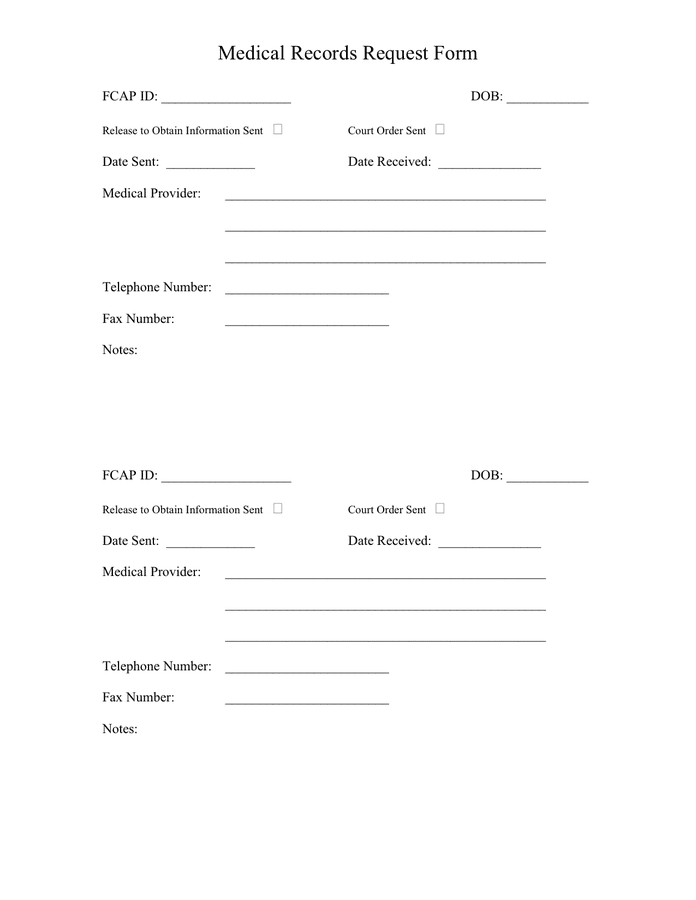
Medical Records Request Form in Word and Pdf formats
The patient’s request must be in writing, signed by the patient, and clearly identify the designated person and where to send the copied records. Patient authorization to transfer or forward dental records i, , hereby request and authorize patient or guardian name (please print).
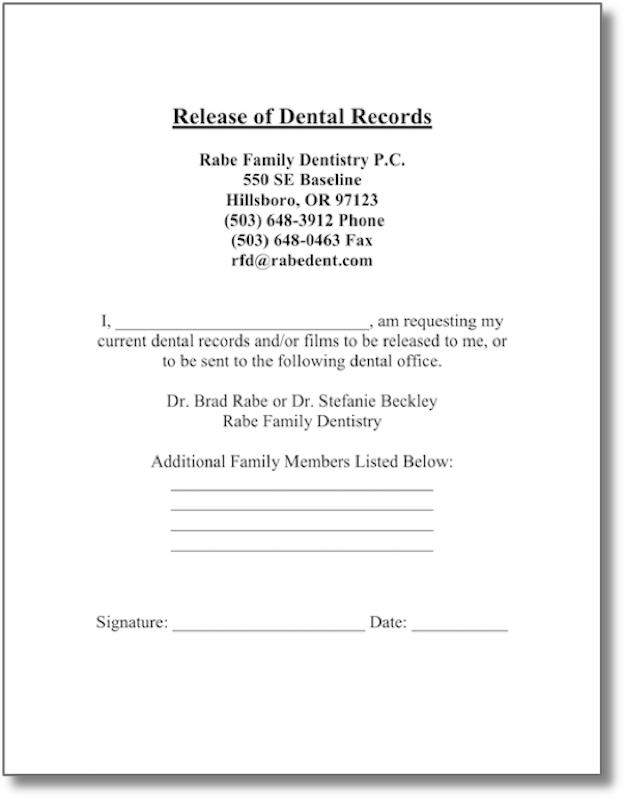
Forms Rabe Family Dentistry
Patient authorization to transfer or forward dental records i, , hereby request and authorize patient or guardian name (please print). The patient’s request must be in writing, signed by the patient, and clearly identify the designated person and where to send the copied records.
Sample Letter Requesting Dental Records Complete with ease airSlate
Patient authorization to transfer or forward dental records i, , hereby request and authorize patient or guardian name (please print). The patient’s request must be in writing, signed by the patient, and clearly identify the designated person and where to send the copied records.

FREE 8+ Sample Dental Records Release Forms in MS Word PDF
Patient authorization to transfer or forward dental records i, , hereby request and authorize patient or guardian name (please print). The patient’s request must be in writing, signed by the patient, and clearly identify the designated person and where to send the copied records.
Printable Dental Lab Case Log Sheet
Patient authorization to transfer or forward dental records i, , hereby request and authorize patient or guardian name (please print). The patient’s request must be in writing, signed by the patient, and clearly identify the designated person and where to send the copied records.
FREE 8+ Sample Dental Records Release Forms in MS Word PDF
The patient’s request must be in writing, signed by the patient, and clearly identify the designated person and where to send the copied records. Patient authorization to transfer or forward dental records i, , hereby request and authorize patient or guardian name (please print).
FREE 8+ Sample Dental Records Release Forms in MS Word PDF
The patient’s request must be in writing, signed by the patient, and clearly identify the designated person and where to send the copied records. Patient authorization to transfer or forward dental records i, , hereby request and authorize patient or guardian name (please print).
The Patient’s Request Must Be In Writing, Signed By The Patient, And Clearly Identify The Designated Person And Where To Send The Copied Records.
Patient authorization to transfer or forward dental records i, , hereby request and authorize patient or guardian name (please print).