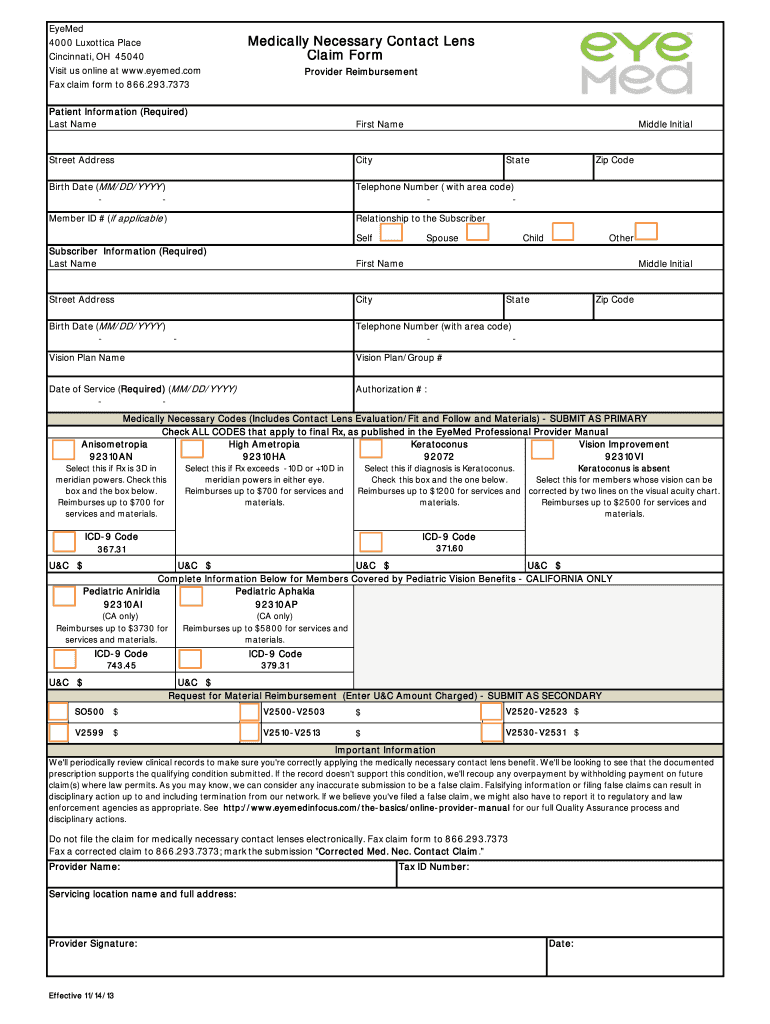
Eyemed Medically Necessary Contacts Form - Contact claim. we'll periodically review clinical records to. Mark the submission corrected med. You need to attach itemized paid. Fax a corrected claim to 866.293.7373; Choose the appropriate codes for the. Download and fill out this form to request reimbursement for medically necessary contact lenses.
Contact claim. we'll periodically review clinical records to. You need to attach itemized paid. Fax a corrected claim to 866.293.7373; Mark the submission corrected med. Download and fill out this form to request reimbursement for medically necessary contact lenses. Choose the appropriate codes for the.
Contact claim. we'll periodically review clinical records to. You need to attach itemized paid. Fax a corrected claim to 866.293.7373; Choose the appropriate codes for the. Download and fill out this form to request reimbursement for medically necessary contact lenses. Mark the submission corrected med.

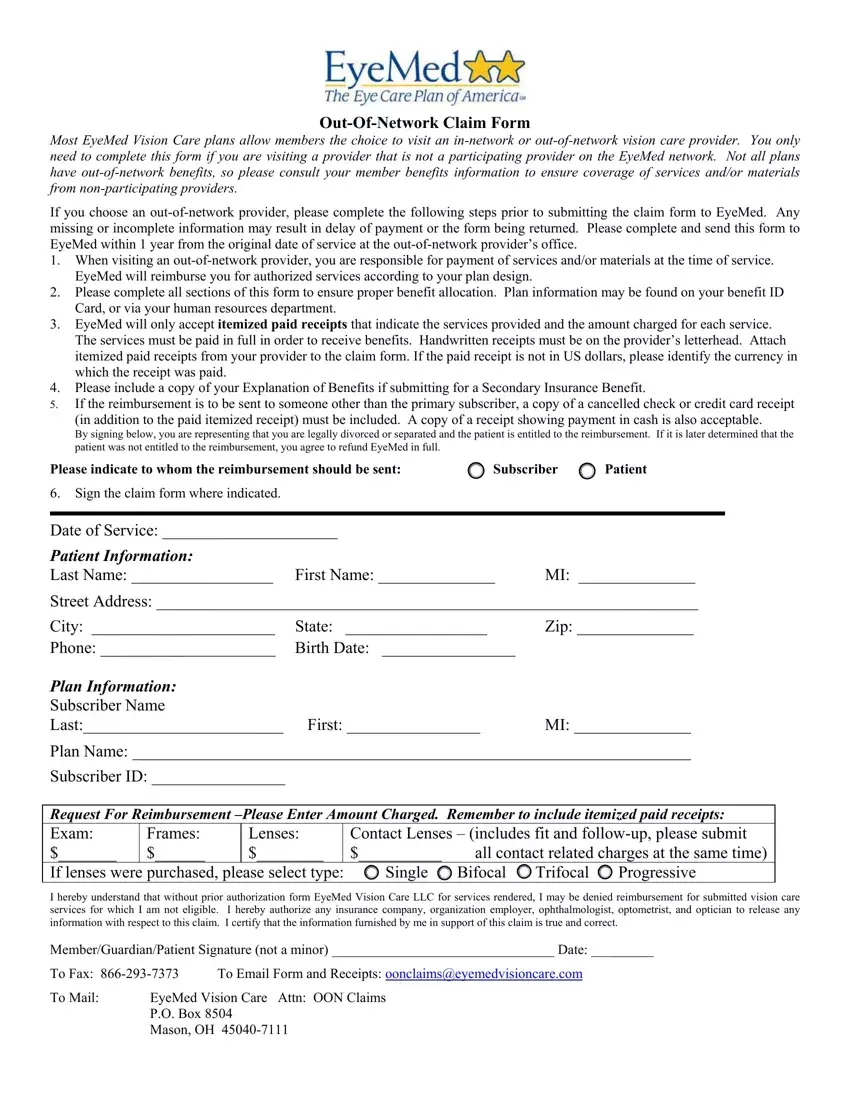
Fillable Online Eyemed Out of Network Claim Form pdf Fax Email Print
Fax a corrected claim to 866.293.7373; Download and fill out this form to request reimbursement for medically necessary contact lenses. You need to attach itemized paid. Choose the appropriate codes for the. Contact claim. we'll periodically review clinical records to.
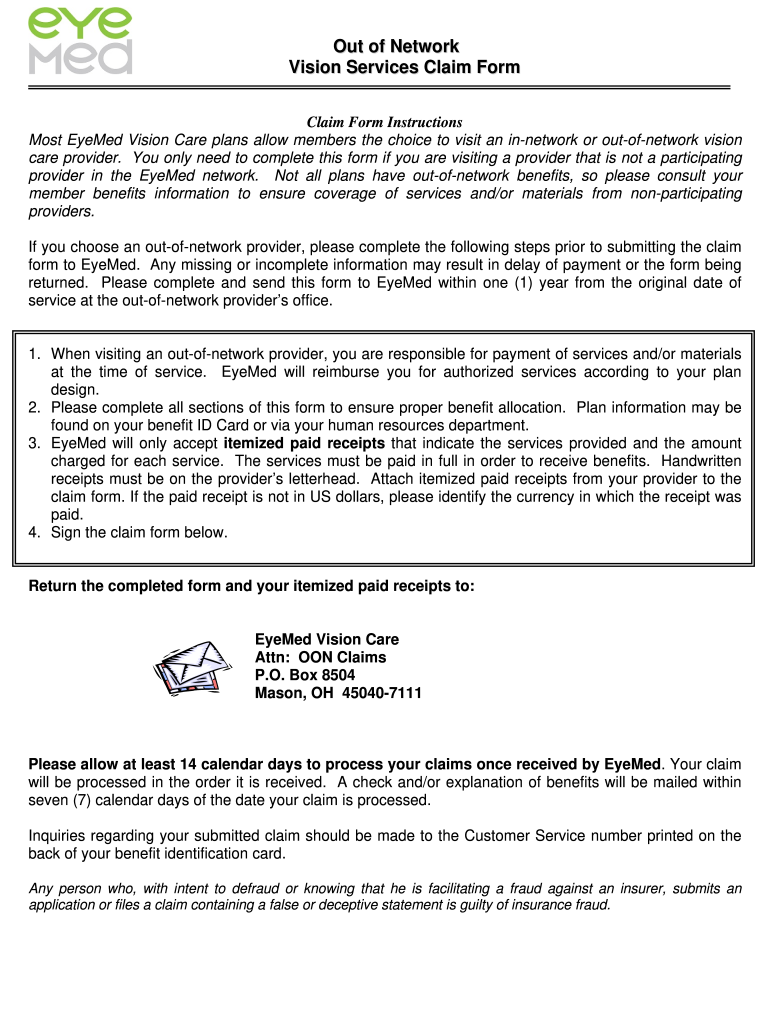
Eyemed Claims Address Fill Online, Printable, Fillable, Blank pdfFiller
Contact claim. we'll periodically review clinical records to. Download and fill out this form to request reimbursement for medically necessary contact lenses. Choose the appropriate codes for the. Fax a corrected claim to 866.293.7373; You need to attach itemized paid.
.jpg)
DACHSER USA/Americas 2019 Benefits. ppt download
Mark the submission corrected med. Download and fill out this form to request reimbursement for medically necessary contact lenses. Fax a corrected claim to 866.293.7373; You need to attach itemized paid. Choose the appropriate codes for the.

Check out your EyeMed membersonly special offers Hub
Download and fill out this form to request reimbursement for medically necessary contact lenses. Mark the submission corrected med. You need to attach itemized paid. Contact claim. we'll periodically review clinical records to. Fax a corrected claim to 866.293.7373;

EyeMed Vision Care Delta Dental
Contact claim. we'll periodically review clinical records to. You need to attach itemized paid. Download and fill out this form to request reimbursement for medically necessary contact lenses. Fax a corrected claim to 866.293.7373; Mark the submission corrected med.
Eyemed Printable Claim Form Printable Lab
You need to attach itemized paid. Fax a corrected claim to 866.293.7373; Contact claim. we'll periodically review clinical records to. Download and fill out this form to request reimbursement for medically necessary contact lenses. Choose the appropriate codes for the.
Eyemed Claim Form ≡ Fill Out Printable PDF Forms Online
Mark the submission corrected med. Download and fill out this form to request reimbursement for medically necessary contact lenses. You need to attach itemized paid. Choose the appropriate codes for the. Fax a corrected claim to 866.293.7373;

Eyemed Insurance Out Of Network Claim Form Creativmakeup Co
Mark the submission corrected med. Choose the appropriate codes for the. Download and fill out this form to request reimbursement for medically necessary contact lenses. Fax a corrected claim to 866.293.7373; You need to attach itemized paid.

Eyemed Printable Claim Form Printable Lab
You need to attach itemized paid. Choose the appropriate codes for the. Fax a corrected claim to 866.293.7373; Download and fill out this form to request reimbursement for medically necessary contact lenses. Mark the submission corrected med.

Fillable Online Out of network claims EyeMed Vision Benefits Fax
Mark the submission corrected med. Contact claim. we'll periodically review clinical records to. You need to attach itemized paid. Fax a corrected claim to 866.293.7373; Choose the appropriate codes for the.
Fax A Corrected Claim To 866.293.7373;
You need to attach itemized paid. Contact claim. we'll periodically review clinical records to. Download and fill out this form to request reimbursement for medically necessary contact lenses. Mark the submission corrected med.