Orthodontic Release Form - I, _____________________________ hereby request to discontinue my/my child’s orthodontic treatment, and remove all orthodontic appliances, even. Orthodontic treatment requires the full cooperation of the. Patient uncooperative or noncompliant and discontinuation of treatment is in his/her best interest. I further acknowledge that said doctor has advised me against removal of said appliances at this time,.
Patient uncooperative or noncompliant and discontinuation of treatment is in his/her best interest. Orthodontic treatment requires the full cooperation of the. I further acknowledge that said doctor has advised me against removal of said appliances at this time,. I, _____________________________ hereby request to discontinue my/my child’s orthodontic treatment, and remove all orthodontic appliances, even.
Patient uncooperative or noncompliant and discontinuation of treatment is in his/her best interest. Orthodontic treatment requires the full cooperation of the. I further acknowledge that said doctor has advised me against removal of said appliances at this time,. I, _____________________________ hereby request to discontinue my/my child’s orthodontic treatment, and remove all orthodontic appliances, even.
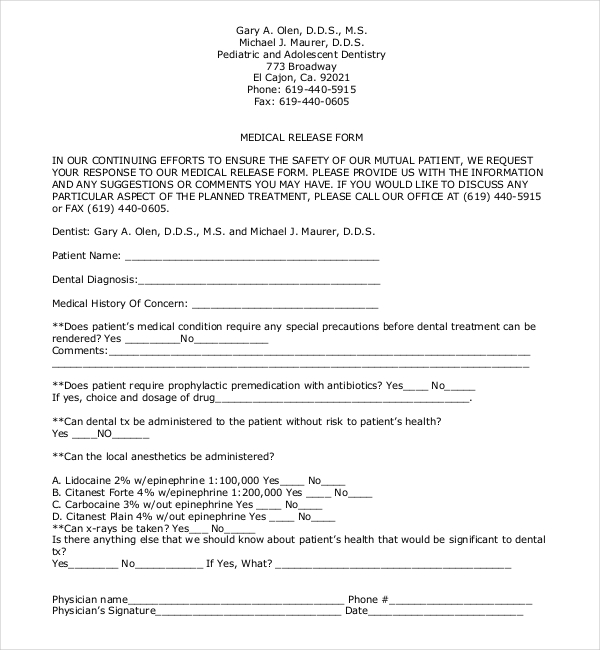
FREE 22+ Sample Medical Release Forms in PDF Word Excel
I further acknowledge that said doctor has advised me against removal of said appliances at this time,. Patient uncooperative or noncompliant and discontinuation of treatment is in his/her best interest. I, _____________________________ hereby request to discontinue my/my child’s orthodontic treatment, and remove all orthodontic appliances, even. Orthodontic treatment requires the full cooperation of the.
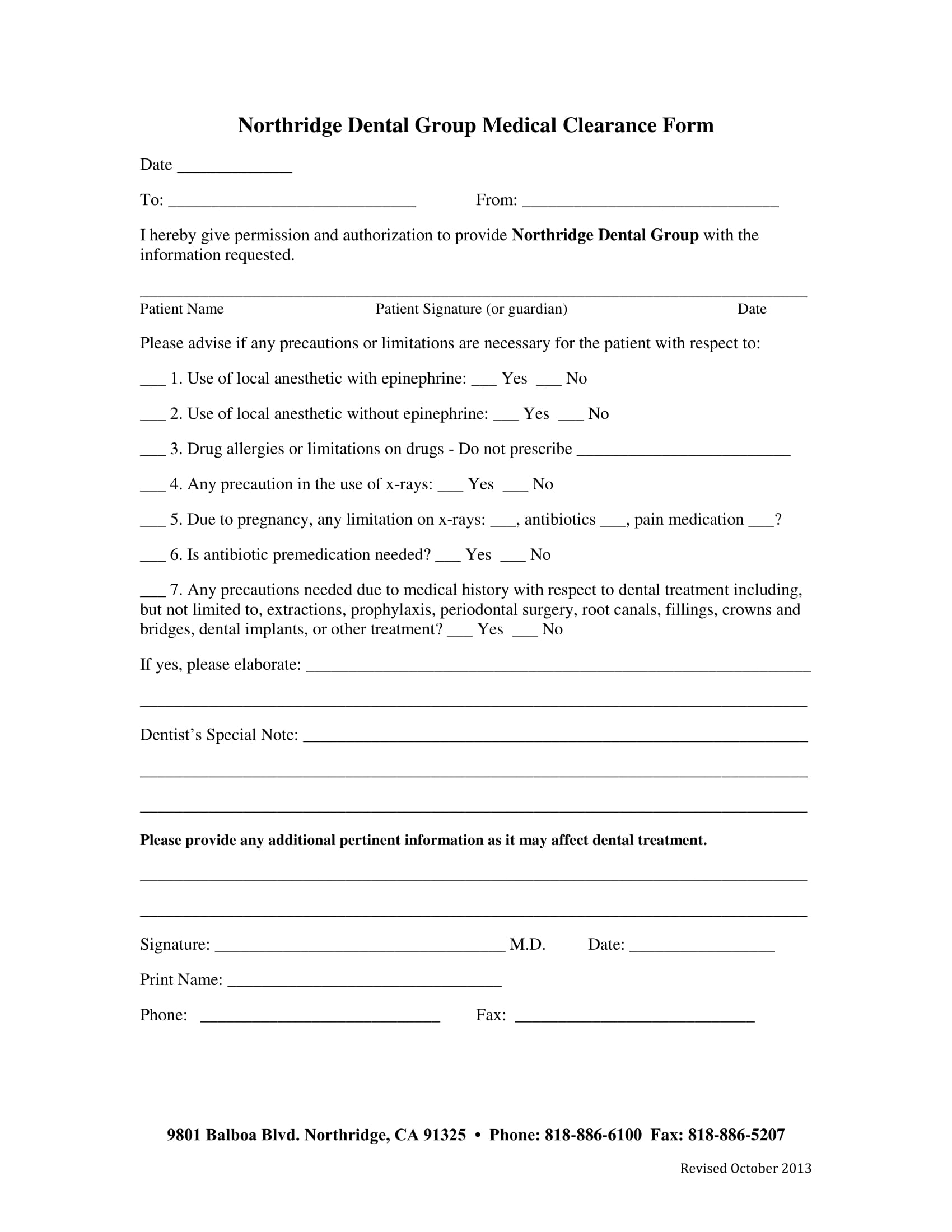
Printable Medical Clearance Form For Dental Treatment
I further acknowledge that said doctor has advised me against removal of said appliances at this time,. Orthodontic treatment requires the full cooperation of the. I, _____________________________ hereby request to discontinue my/my child’s orthodontic treatment, and remove all orthodontic appliances, even. Patient uncooperative or noncompliant and discontinuation of treatment is in his/her best interest.
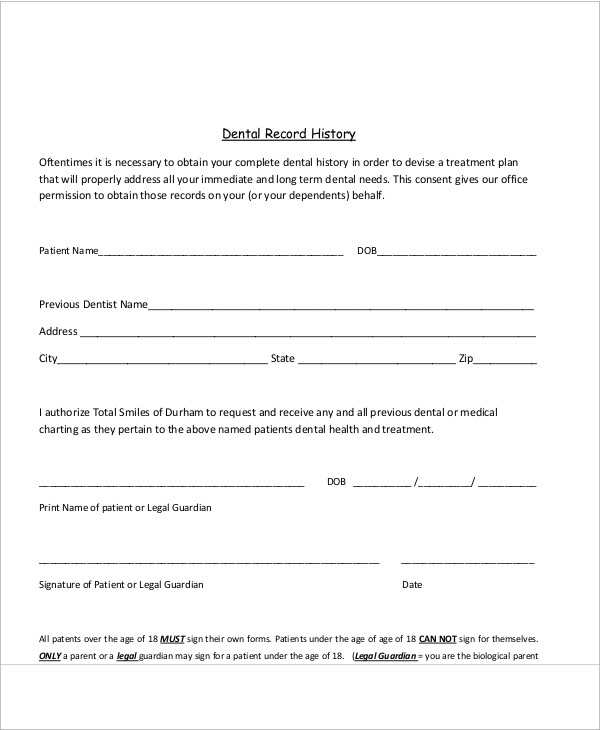
FREE 11+ Sample Dental Release Forms in MS Word PDF
I, _____________________________ hereby request to discontinue my/my child’s orthodontic treatment, and remove all orthodontic appliances, even. Patient uncooperative or noncompliant and discontinuation of treatment is in his/her best interest. I further acknowledge that said doctor has advised me against removal of said appliances at this time,. Orthodontic treatment requires the full cooperation of the.
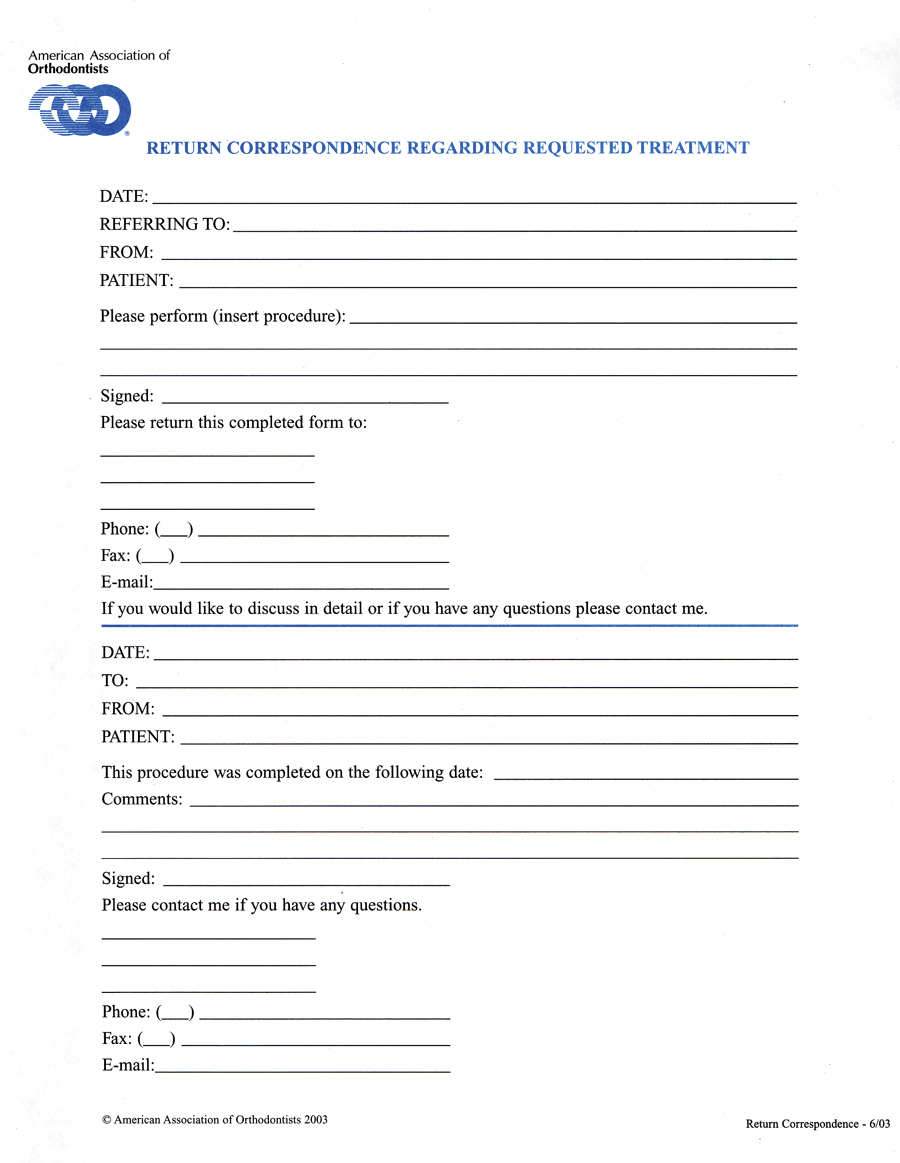
Aao Transfer Form Printable Printable Forms Free Online
I further acknowledge that said doctor has advised me against removal of said appliances at this time,. Patient uncooperative or noncompliant and discontinuation of treatment is in his/her best interest. Orthodontic treatment requires the full cooperation of the. I, _____________________________ hereby request to discontinue my/my child’s orthodontic treatment, and remove all orthodontic appliances, even.
FREE 11+ Sample Dental Release Forms in MS Word PDF
Orthodontic treatment requires the full cooperation of the. Patient uncooperative or noncompliant and discontinuation of treatment is in his/her best interest. I further acknowledge that said doctor has advised me against removal of said appliances at this time,. I, _____________________________ hereby request to discontinue my/my child’s orthodontic treatment, and remove all orthodontic appliances, even.

Concerns About Your Child's Ortho Health Prettyman Orthodontics
I, _____________________________ hereby request to discontinue my/my child’s orthodontic treatment, and remove all orthodontic appliances, even. Orthodontic treatment requires the full cooperation of the. I further acknowledge that said doctor has advised me against removal of said appliances at this time,. Patient uncooperative or noncompliant and discontinuation of treatment is in his/her best interest.
Early Removal Of Braces Consent Form Fill Online, Printable, Fillable
Patient uncooperative or noncompliant and discontinuation of treatment is in his/her best interest. I, _____________________________ hereby request to discontinue my/my child’s orthodontic treatment, and remove all orthodontic appliances, even. Orthodontic treatment requires the full cooperation of the. I further acknowledge that said doctor has advised me against removal of said appliances at this time,.

Dental XRay Release Form Template Word PDF Google Docs Highfile
I further acknowledge that said doctor has advised me against removal of said appliances at this time,. Patient uncooperative or noncompliant and discontinuation of treatment is in his/her best interest. Orthodontic treatment requires the full cooperation of the. I, _____________________________ hereby request to discontinue my/my child’s orthodontic treatment, and remove all orthodontic appliances, even.

Authorization To Release Dental Information Printable Pdf Download
I, _____________________________ hereby request to discontinue my/my child’s orthodontic treatment, and remove all orthodontic appliances, even. I further acknowledge that said doctor has advised me against removal of said appliances at this time,. Orthodontic treatment requires the full cooperation of the. Patient uncooperative or noncompliant and discontinuation of treatment is in his/her best interest.
FREE 6+ Dental Records Release Forms in PDF MS Word
Orthodontic treatment requires the full cooperation of the. I further acknowledge that said doctor has advised me against removal of said appliances at this time,. I, _____________________________ hereby request to discontinue my/my child’s orthodontic treatment, and remove all orthodontic appliances, even. Patient uncooperative or noncompliant and discontinuation of treatment is in his/her best interest.
I Further Acknowledge That Said Doctor Has Advised Me Against Removal Of Said Appliances At This Time,.
Patient uncooperative or noncompliant and discontinuation of treatment is in his/her best interest. Orthodontic treatment requires the full cooperation of the. I, _____________________________ hereby request to discontinue my/my child’s orthodontic treatment, and remove all orthodontic appliances, even.