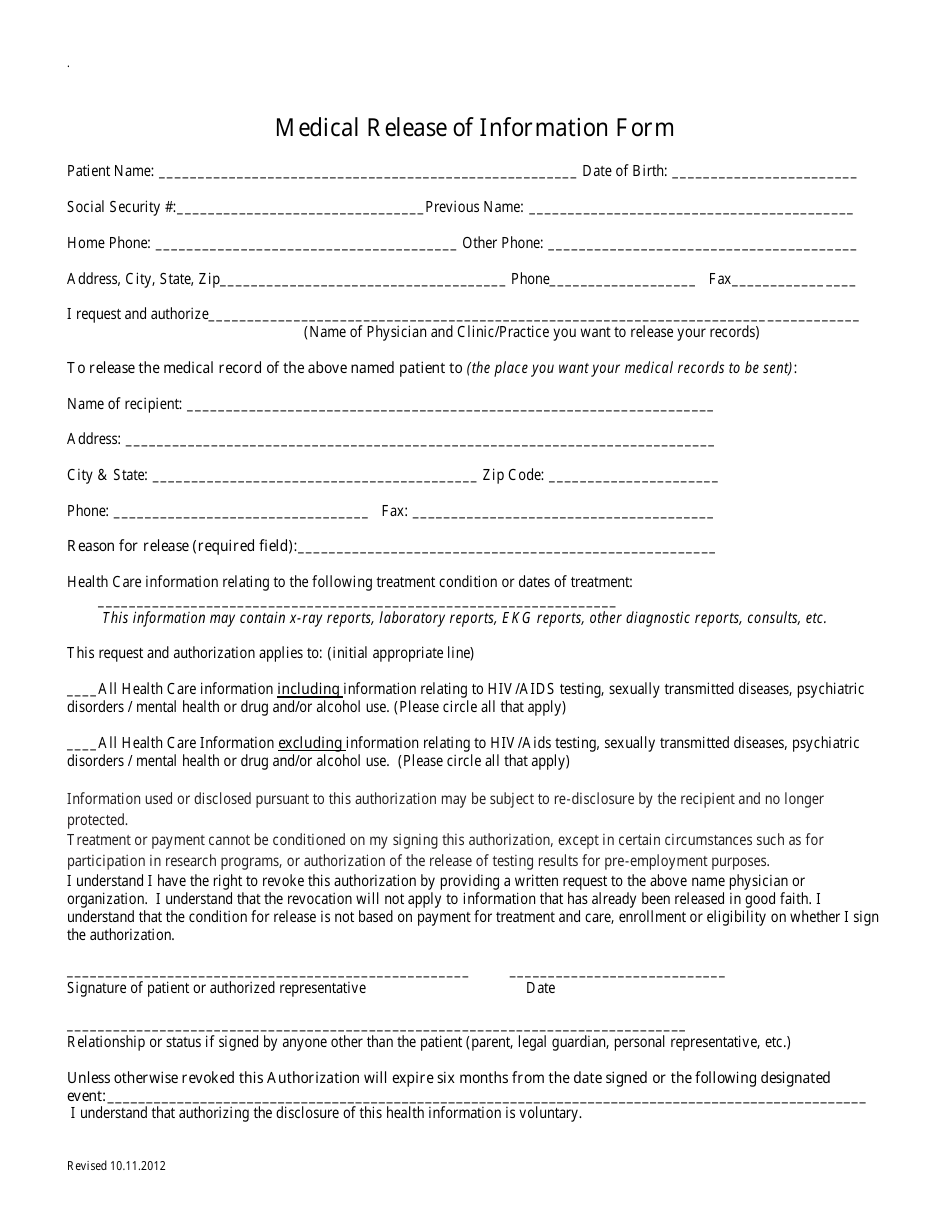
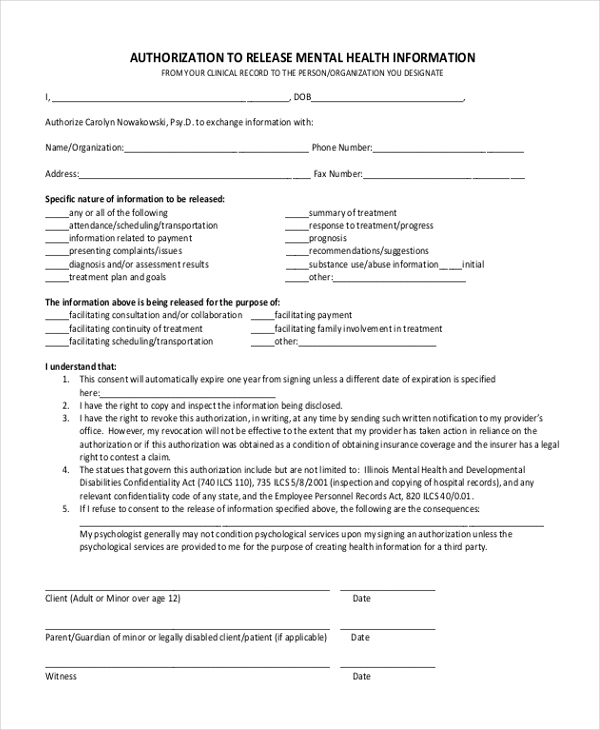
Release Of Information Form Mental Health Template - Full treatment record including all health/mental. To release, discuss, or disclose the following: The purpose of this disclosure of information is to improve assessment and treatment planning, share information relevant to treatment and when. Full treatment record excluding the following information: The protected health information to be. This form provides your therapist with written permission to communicate with other individual providers regarding your treatment (e.g. Information necessary to identify, diagnose, prognosis, or treatment for mental health, substance abuse (alcohol/drug use), and any other relevant. I, the undersigned, understand that a copy of this signed authorization form is as acceptable as the original.
Information necessary to identify, diagnose, prognosis, or treatment for mental health, substance abuse (alcohol/drug use), and any other relevant. To release, discuss, or disclose the following: The protected health information to be. Full treatment record including all health/mental. This form provides your therapist with written permission to communicate with other individual providers regarding your treatment (e.g. Full treatment record excluding the following information: I, the undersigned, understand that a copy of this signed authorization form is as acceptable as the original. The purpose of this disclosure of information is to improve assessment and treatment planning, share information relevant to treatment and when.
Information necessary to identify, diagnose, prognosis, or treatment for mental health, substance abuse (alcohol/drug use), and any other relevant. The protected health information to be. This form provides your therapist with written permission to communicate with other individual providers regarding your treatment (e.g. To release, discuss, or disclose the following: Full treatment record excluding the following information: The purpose of this disclosure of information is to improve assessment and treatment planning, share information relevant to treatment and when. I, the undersigned, understand that a copy of this signed authorization form is as acceptable as the original. Full treatment record including all health/mental.
Medical Release of Information Form Fill Out, Sign Online and
The purpose of this disclosure of information is to improve assessment and treatment planning, share information relevant to treatment and when. Information necessary to identify, diagnose, prognosis, or treatment for mental health, substance abuse (alcohol/drug use), and any other relevant. I, the undersigned, understand that a copy of this signed authorization form is as acceptable as the original. To release,.
Release Of Information Template Free
This form provides your therapist with written permission to communicate with other individual providers regarding your treatment (e.g. Full treatment record excluding the following information: To release, discuss, or disclose the following: I, the undersigned, understand that a copy of this signed authorization form is as acceptable as the original. The protected health information to be.
Mental Health Release Of Information Template
Full treatment record including all health/mental. To release, discuss, or disclose the following: Information necessary to identify, diagnose, prognosis, or treatment for mental health, substance abuse (alcohol/drug use), and any other relevant. Full treatment record excluding the following information: This form provides your therapist with written permission to communicate with other individual providers regarding your treatment (e.g.

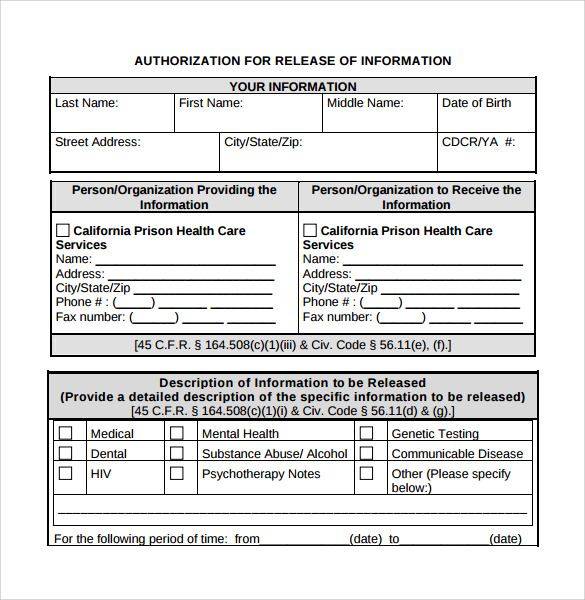
Mental Health Release Of Information Form California
To release, discuss, or disclose the following: Full treatment record including all health/mental. The protected health information to be. The purpose of this disclosure of information is to improve assessment and treatment planning, share information relevant to treatment and when. Full treatment record excluding the following information:

Free Counseling Release Of Information Form Template Pdf Example Posted
To release, discuss, or disclose the following: Full treatment record excluding the following information: This form provides your therapist with written permission to communicate with other individual providers regarding your treatment (e.g. Full treatment record including all health/mental. I, the undersigned, understand that a copy of this signed authorization form is as acceptable as the original.

Printable Mental Health Release Form
Information necessary to identify, diagnose, prognosis, or treatment for mental health, substance abuse (alcohol/drug use), and any other relevant. The protected health information to be. To release, discuss, or disclose the following: Full treatment record excluding the following information: The purpose of this disclosure of information is to improve assessment and treatment planning, share information relevant to treatment and when.
FREE 22+ Release of Information Form Samples, PDF, MS Word, Google Docs
The protected health information to be. To release, discuss, or disclose the following: The purpose of this disclosure of information is to improve assessment and treatment planning, share information relevant to treatment and when. Full treatment record excluding the following information: Information necessary to identify, diagnose, prognosis, or treatment for mental health, substance abuse (alcohol/drug use), and any other relevant.
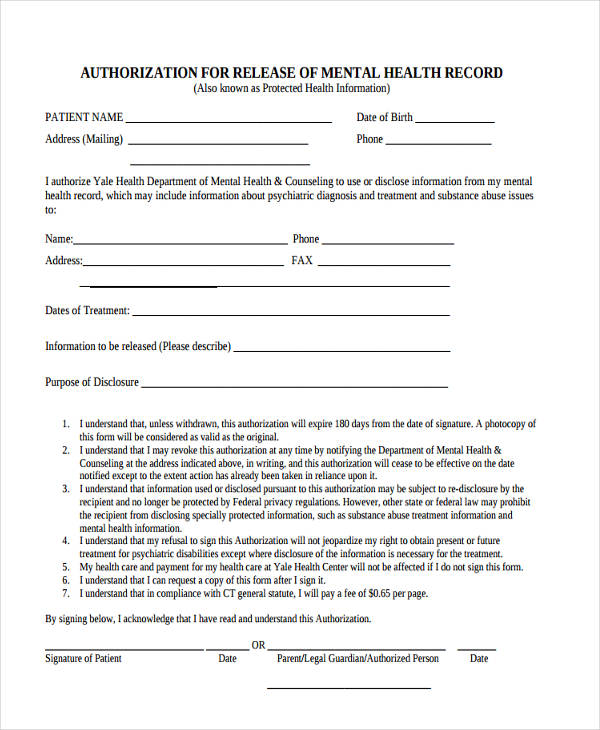
Free Mental Health Release Of Information Form
This form provides your therapist with written permission to communicate with other individual providers regarding your treatment (e.g. To release, discuss, or disclose the following: Full treatment record excluding the following information: I, the undersigned, understand that a copy of this signed authorization form is as acceptable as the original. The protected health information to be.
Free Release Of Information Form Mental Health Template Doc
I, the undersigned, understand that a copy of this signed authorization form is as acceptable as the original. Full treatment record excluding the following information: To release, discuss, or disclose the following: Full treatment record including all health/mental. The purpose of this disclosure of information is to improve assessment and treatment planning, share information relevant to treatment and when.
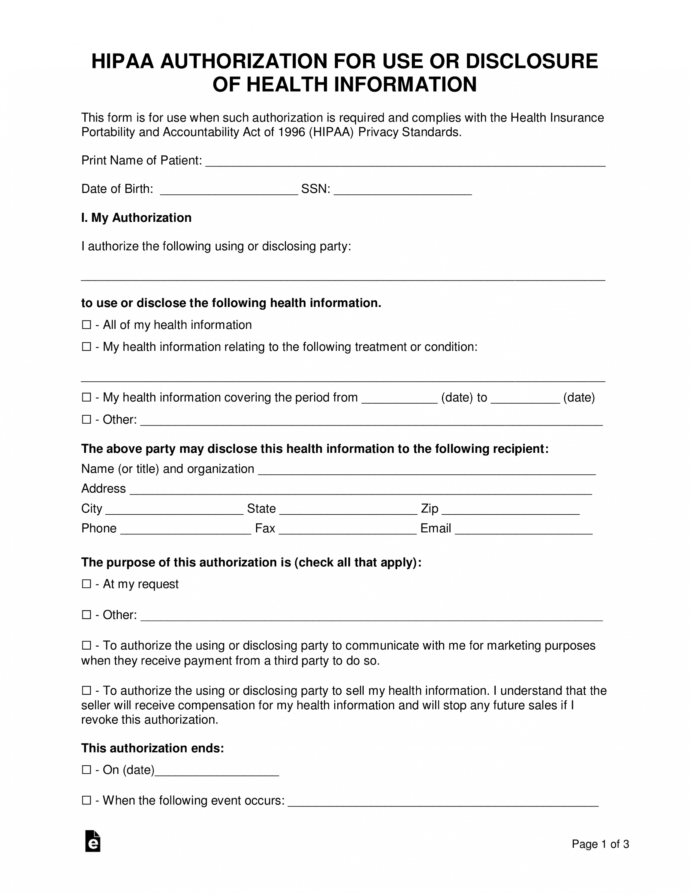
Best HIPAA Release Guide Free 2023 HIPAA Compliant Authorization Form
Information necessary to identify, diagnose, prognosis, or treatment for mental health, substance abuse (alcohol/drug use), and any other relevant. This form provides your therapist with written permission to communicate with other individual providers regarding your treatment (e.g. The purpose of this disclosure of information is to improve assessment and treatment planning, share information relevant to treatment and when. The protected.
I, The Undersigned, Understand That A Copy Of This Signed Authorization Form Is As Acceptable As The Original.
The purpose of this disclosure of information is to improve assessment and treatment planning, share information relevant to treatment and when. This form provides your therapist with written permission to communicate with other individual providers regarding your treatment (e.g. Full treatment record excluding the following information: To release, discuss, or disclose the following:
Full Treatment Record Including All Health/Mental.
Information necessary to identify, diagnose, prognosis, or treatment for mental health, substance abuse (alcohol/drug use), and any other relevant. The protected health information to be.