Dentaquest Non Covered Services Form - The member or the member's legal representative hereby acknowledges that he or she has been informed that the following health care services to. Service(s) not paid for by the benefit plan (practice name) accepts (plan name) dental benefit plan, under which you are covered:. What can i do if dentaquest denies or limits my member’s request for a covered service? “customer” is any individual who is enrolled in the illinois medicaid or hfs dental. “covered service” is a service for which payment can be made. 23 how will i find out if services are denied?.
What can i do if dentaquest denies or limits my member’s request for a covered service? Service(s) not paid for by the benefit plan (practice name) accepts (plan name) dental benefit plan, under which you are covered:. The member or the member's legal representative hereby acknowledges that he or she has been informed that the following health care services to. “customer” is any individual who is enrolled in the illinois medicaid or hfs dental. “covered service” is a service for which payment can be made. 23 how will i find out if services are denied?.
“customer” is any individual who is enrolled in the illinois medicaid or hfs dental. What can i do if dentaquest denies or limits my member’s request for a covered service? 23 how will i find out if services are denied?. The member or the member's legal representative hereby acknowledges that he or she has been informed that the following health care services to. Service(s) not paid for by the benefit plan (practice name) accepts (plan name) dental benefit plan, under which you are covered:. “covered service” is a service for which payment can be made.
Dentaquest Reimbursement Form Complete with ease airSlate SignNow
23 how will i find out if services are denied?. What can i do if dentaquest denies or limits my member’s request for a covered service? “customer” is any individual who is enrolled in the illinois medicaid or hfs dental. The member or the member's legal representative hereby acknowledges that he or she has been informed that the following health.

Fillable Online Medicare NonCovered Continued Stay Form Fax Email
23 how will i find out if services are denied?. Service(s) not paid for by the benefit plan (practice name) accepts (plan name) dental benefit plan, under which you are covered:. “covered service” is a service for which payment can be made. The member or the member's legal representative hereby acknowledges that he or she has been informed that the.

DentaQuest Evolves Business Strategy to Transform Oral Health
The member or the member's legal representative hereby acknowledges that he or she has been informed that the following health care services to. What can i do if dentaquest denies or limits my member’s request for a covered service? Service(s) not paid for by the benefit plan (practice name) accepts (plan name) dental benefit plan, under which you are covered:..

Fillable Online Advance Recipient Notice of Noncovered Service/Item
“covered service” is a service for which payment can be made. The member or the member's legal representative hereby acknowledges that he or she has been informed that the following health care services to. Service(s) not paid for by the benefit plan (practice name) accepts (plan name) dental benefit plan, under which you are covered:. What can i do if.
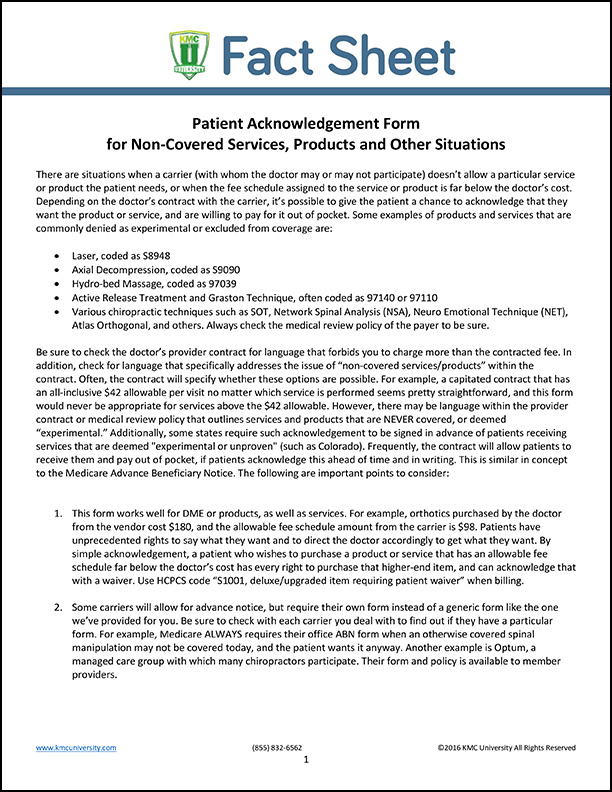
Patient Acknowledgement Form for NonCovered Services, Products and
“covered service” is a service for which payment can be made. The member or the member's legal representative hereby acknowledges that he or she has been informed that the following health care services to. 23 how will i find out if services are denied?. What can i do if dentaquest denies or limits my member’s request for a covered service?.

Fillable Online NONCOVERED SERVICES AGREEMENT Fax Email Print pdfFiller
“customer” is any individual who is enrolled in the illinois medicaid or hfs dental. What can i do if dentaquest denies or limits my member’s request for a covered service? “covered service” is a service for which payment can be made. Service(s) not paid for by the benefit plan (practice name) accepts (plan name) dental benefit plan, under which you.
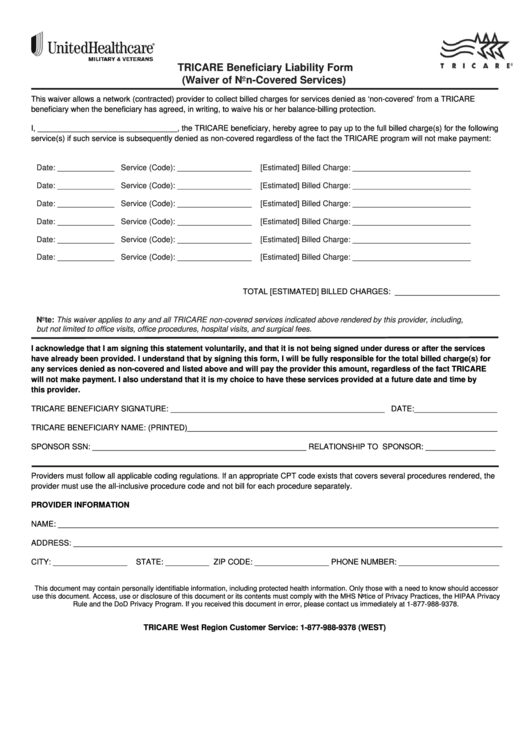
Fillable Tricare Beneficiary Liability Form (Waiver Of NonCovered
“covered service” is a service for which payment can be made. Service(s) not paid for by the benefit plan (practice name) accepts (plan name) dental benefit plan, under which you are covered:. “customer” is any individual who is enrolled in the illinois medicaid or hfs dental. The member or the member's legal representative hereby acknowledges that he or she has.

Fillable Online Medicare Dental Reimbursement Form DentaQuest Fax
“covered service” is a service for which payment can be made. Service(s) not paid for by the benefit plan (practice name) accepts (plan name) dental benefit plan, under which you are covered:. The member or the member's legal representative hereby acknowledges that he or she has been informed that the following health care services to. 23 how will i find.

Dentaquest Fee Schedule 2024 Roz Leshia
“customer” is any individual who is enrolled in the illinois medicaid or hfs dental. 23 how will i find out if services are denied?. The member or the member's legal representative hereby acknowledges that he or she has been informed that the following health care services to. What can i do if dentaquest denies or limits my member’s request for.

Fillable Online Dentaquest Provider Change Form. Dentaquest Provider
“covered service” is a service for which payment can be made. 23 how will i find out if services are denied?. “customer” is any individual who is enrolled in the illinois medicaid or hfs dental. What can i do if dentaquest denies or limits my member’s request for a covered service? The member or the member's legal representative hereby acknowledges.
What Can I Do If Dentaquest Denies Or Limits My Member’s Request For A Covered Service?
“covered service” is a service for which payment can be made. “customer” is any individual who is enrolled in the illinois medicaid or hfs dental. Service(s) not paid for by the benefit plan (practice name) accepts (plan name) dental benefit plan, under which you are covered:. 23 how will i find out if services are denied?.